1. Introduction
Due to the spread of COVID-19 infection worldwide and the resulting mortality, as well as the lack of a definitive treatment for it, various non-invasive and invasive drugs and treatments around the world have been used to mitigate the effects of the disease or accelerate the treatment process. However, the positive and definite effect of none of these cases has been confirmed and they have been effective only in some cases. Recent studies showed that obesity, high blood pressure, diabetes, and heart failure make it difficult to treat COVID-19. In this study, some clinical features and the need for supportive therapies in patients died due to COVID-19 were investigated to provide useful solutions for targeted recovery for patients.
2. Materials and Methods
This is an applied, descriptive-analytical retrospective study conducted on 100 COVID-19 patients who died in Hajar Hospital in Tehran, Iran from February to September 2020 who were selected using a census method. They were divided into two groups of with and without underlying disease. After coordination and obtaining the necessary permission and informed consent from the head of the intensive care unit, and visiting Hajar Hospital with full observance of infection control standards and full personal protection coverage, Information (Age, gender, the need for any of the supportive treatments during the hospitalization period) was collected from the medial files of samples. The patients with positive CT scan (lung scan) and PCR test who died of COVID-19 were included in the study. The criterion for excluding from the study was the death caused by other diseases. The course of the disease is classified into zero stage (with no symptoms), symptom onset stage, respiratory infection stage which is divided into two levels of moderate and severe, and finally the stage of severe and critical inflammation. The final stage is the criterion for entering supportive treatment where the patient needs special care. Criteria for entering this stage were at least one of the following cases: respiratory failure, blood oxygen saturation (SpO2) <90%, shock symptoms, need for mechanical ventilation or multiple organ failure. Mortality rates in the intensive care unit varies depending on the underlying disease. If necessary, according to the physician’s advice and the patient’s special condition, special supportive treatments are used. Statistical analysis was performed in SPSS v. 22 software using independent t-test to investigate quantitative variables with normal distribution. The significance level was set at 0.05.
3. Results
According to the results, 52(52%) of the deceased were male (mean age= 70 years) and 48(48%) were female (mean age= 73 years). The deceased patients aged 36-96 years. During the hospitalization period, 62 patients (62%) required mechanical ventilation through artificial respiration, 28(28%) required injection of vasoconstrictor, and 13(13%) required blood product injection. The mortality rate was 25(25%) in winter, 37(37%) in spring and 38(38%) in summer. There was no significant difference in age and gender between the two groups (p≥0.05). The age and gender showed no significant relationship with the need for supportive treatments (p≥0.05), but had a significant relationship with underlying disease (p<0.05). Rapid progression of respiratory symptoms, respiratory Rate > 30 per minute (with or without fever), shortness of breath, SpO2<90 in room temperature, and increased lung involvement by more than 50% were reported on CT scan of the deceased patients (P=0.01). These patients had entered a critical stage of disease progression. At this stage, the patient needs special care. Severe types of disease can occur at any time during the course of the disease and its occurrence does not necessarily require all previous and early stages of the disease. Patients with refractory hypoxemia, decreased level of consciousness, instability of blood flow and increased carbon monoxide in the blood with respiratory fatigue had been admitted to the intensive care unit. The cause of death was reported to be lack of contraction of the heart muscle and lack of output and blood flow in the heart or asystole.
Figure 1 shows data on deceased patients’ need for supportive care. Statistical analysis of their data showed that the use of mechanical ventilation (n=62, 62%) was significantly higher than other supportive methods (p=0.01).
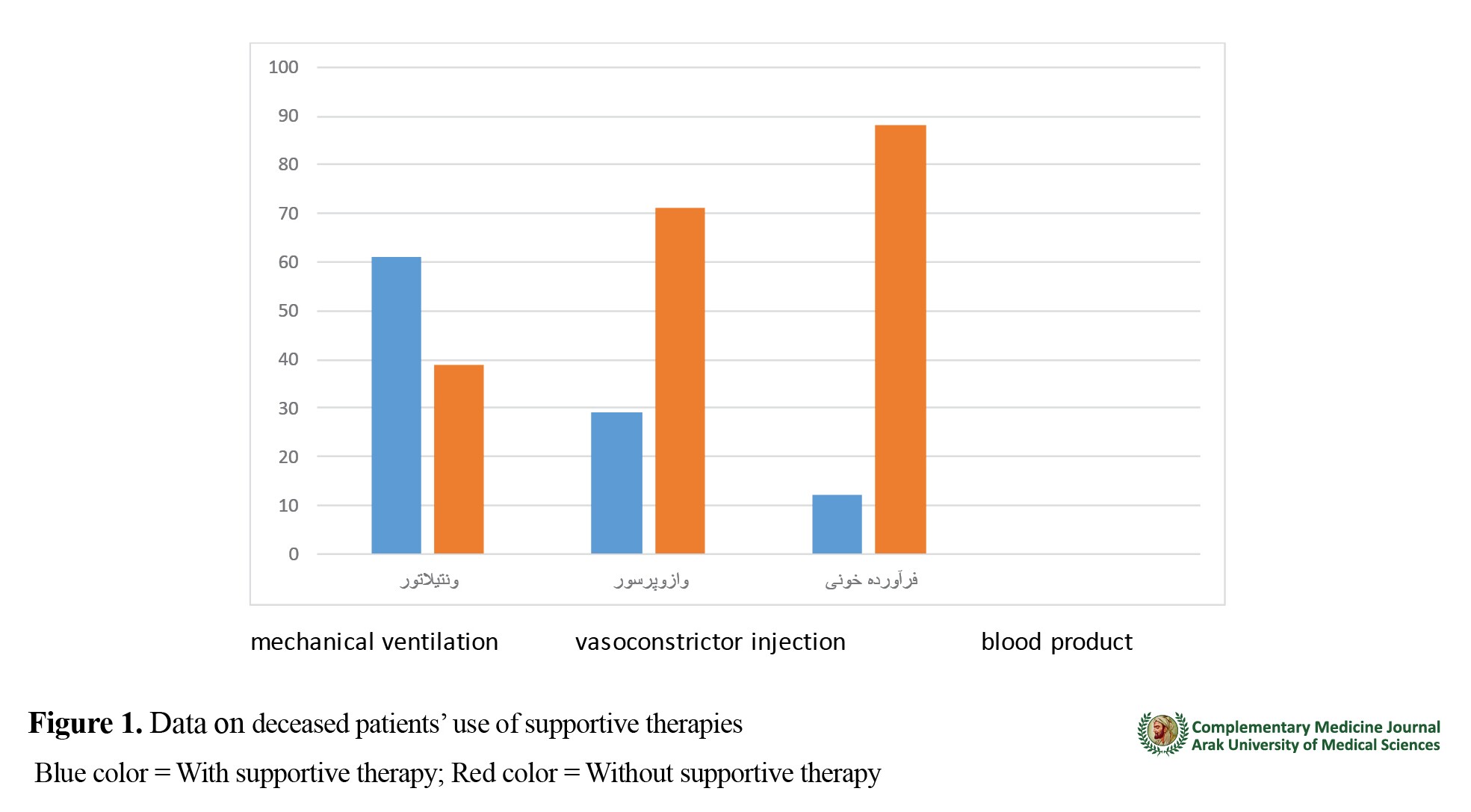
It should be noted that two or more supportive therapies had not been used together. As can be seen in
Figure 2, most of deceased patients had an underlying disease. Ventilators were used in 69 patients (69%) with underlying diseases and 31 patients (31%) without underlying diseases.

The most common underlying diseases were high blood pressure, diabetes and heart problems. The severity of the disease and clinical manifestations and the mortality rate of patients with cardiovascular disease, diabetes and hypertension were significantly different than those with other underlying diseases (p=0.01) (
Figure 3).

Ethical Considerations
Compliance with ethical guidelines
This study was conducted in accordance with ethical principles in medical research on humans (Helsinki Declaration). Ethical approval was obtained from the Ethics Committee of Aja University of Medical Sciences (Code: IR.AJAUMS.REC.1399.069).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally in preparing this article
Conflicts of interest
The authors declare no conflict of interest
Acknowledgements
The authors would like to thank Iran University of Medical Sciences and AJA University of Medical Sciences for their financial support and Hajar Hospital for specialized tests
References
- Emanuel EJ, Persad G, Upshur R, Thome P, Parker M, Glickman A, et al. Fair allocation of scarce medical resources in the time of Covid-19. The New England Journal of Medicine. 2020; 382:2049-2055. [DOI:10.1056/NEJMsb2005114] [PMID]
- Arentz M, Yim E, Klaff L, Lokhandwala S, Riedo FX, Chong M, et al. Characteristics and outcomes of 21 critically ill patients with COVID-19 in Washington State. JAMA. 2020; 323(16):1612-4. [DOI:10.1001/jama.2020.4326] [PMID] [PMCID]
- Biddison LD, Berkowitz KA, Courtney B, De Jong CM, Devereaux AV, Kissoon N, et al. Ethical considerations: care of the critically ill and injured during pandemics and disasters: CHEST consensus statement. Chest. 2014; 146(4):e145S-55S. [DOI:10.1378/chest.14-0742] [PMID]
- Phua J, Weng L, Ling L, Egi M, Lim CM, Divatia JV, et al. Intensive care management of Coronavirus Disease 2019 (COVID-19): Challenges and recommendations. The Lancet Respiratory Medicine. 2020; 8(5):506-17. [DOI:10.1016/S2213-2600(20)30161-2]
- Alhazzani W, Møller MH, Arabi YM, Loeb M, Gong MN, Fan E, et al. Surviving sepsis campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Medicine. 2020; 46(5):854-87. [DOI:10.1007/s00134-020-06022-5] [PMID] [PMCID]
- Gattinoni L, Coppola S, Cressoni M, Busana M, Rossi S, Chiumello D. COVID-19 does not lead to a “typical” acute respiratory distress syndrome. American Journal of Respiratory and Critical Care Medicine. 2020; 201(10):1299-300. [DOI:10.1164/rccm.202003-0817LE] [PMID] [PMCID]
- Gattinoni L, Chiumello D, Caironi P, Busana M, Romitti F, Brazzi L, Camporota L. COVID-19 pneumonia: different respiratory treatments for different phenotypes? Intensive Care Medicine. 2020; 46:1099–102. [DOI:10.1007/s00134-020-06033-2] [PMID] [PMCID]
- Yang X, Yu Y, Xu J, Shu H, Liu H, Wu Y, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. The Lancet Respiratory Medicine. 2020; 8(5):475-81. [DOI:10.1016/S2213-2600(20)30079-5]
- Prakash D. Anemia in the ICU: Anemia of chronic disease versus anemia of acute illness. Critical Care Clinics. 2012; 28(3):333-43. [DOI:10.1016/j.ccc.2012.04.012] [PMID]
- Vincent JL, Abraham E, Kochanek P, Moore FA, Fink MP. Textbook of critical care e-book. Amsterdam: Elsevier Health Sciences; 2011. https://books.google.com/books?hl=en&lr=&id=uAl68tCzm5IC&oi=fnd&pg=
- Rodriguez RM, Corwin HL, Gettinger A, Corwin MJ, Gubler D, Pearl RG. Nutritional deficiencies and blunted erythropoietin response as causes of the anemia of critical illness. Journal of Critical Care. 2001, 16:3641. [DOI:10.1053/jcrc.2001.21795] [PMID]
- Talebi S, Nematshahi M, Tajabadi A, Khosrogerdi A. [Comparison of clinical and epidemiological characteristics of deceased and recovered patients with COVID-19 in Sabzevar, Iran (Persian)]. Journal Military Medicine. 2020; 22(6):509-16. http://militarymedj.ir/article-1-2580-en.html
- Lal Kheirkhah E, Haddadi M, Ardakani M, Adel Barkhordar A, Taraz Z, Yazdi S. [Clinical demonstrations, laboratory and radiological findings of pediatric patients with COVID-19 in esfarayen-a case series (Persian)]. Journal of Sabzevar University of Medical Sciences. 2021; 27(6):796-800. http://jsums.sinaweb.net/article_1342_0.html?lang=en
- Forbes P, Finch A. Redeployed staff and better teamwork: How COVID-19 has transformed nursing. 2020; 27(4):14-17. [DOI:10.7748/nm.27.4.14.s11]



 , Fatemeh Tabatabaie2
, Fatemeh Tabatabaie2 




